{kind=link}
As WSU trains Native American health-care providers and researchers, Western-style healthcare could be transformed by ancient, time-tested practices.
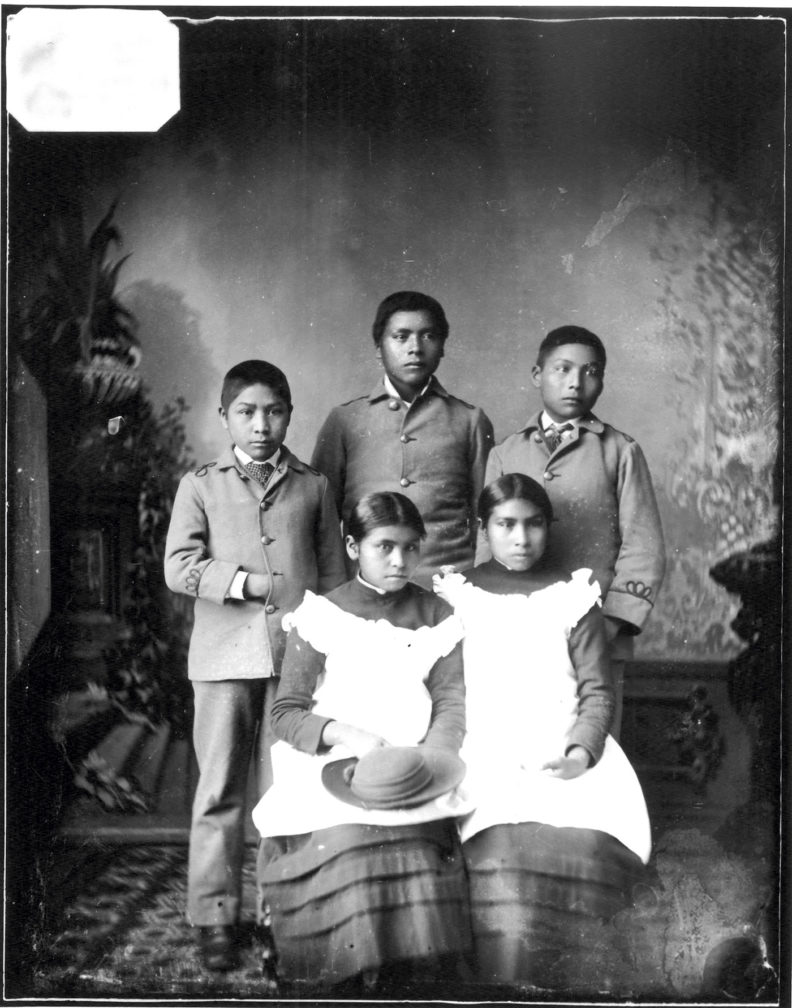
After the War of 1877, Robbie Paul’s grandfather was 10 when, along with six other children, he was shipped from the Nez Perce exile camp in Oklahoma to the new Indian boarding school in Carlisle, Pennsylvania. As her grandfather parted with his mother that day in 1880, mother said to son: go, learn what you can, then come back to us. And, Paul thinks, based on a healing dream she had, the boy’s mother perhaps discreetly slipped a medicine bag into his coat, something to keep his feet on the same earth as hers.
In a photo Paul still has, her grandfather, posed with his few other Nez Perce schoolmates, has his hand inside his coat. She thinks he’s clutching the medicine bag, holding on, in a sense, for dear life, and that kept him together, body and soul, for the years he was in boarding school. He did come home in July 1888, and he still spoke fluent Nez Perce.
Paul, too, spent time in a boarding school, as did her father before her. “In essence,” she says, “I’m still healing, so that’s what I speak about.”
Paul, Washington State University’s retired director of Native American Health Sciences, is writing a history of her Nez Perce family, and an exhibit of her family’s archives—including her grandfather’s trunk from boarding school days—opened at WSU’s Manuscripts, Archives, and Special Collections in October.

The Indian boarding schools damaged generations of people with their philosophy of extreme assimilation. The system’s founder, Richard Pratt, said, you have to “kill the Indian” in order to “save the Man.” This pedagogy of oppression stripped multiple consecutive generations of North American indigenous people of their names, families, languages, stories, cultures, and land. Their medicine bags were outlawed, too.
Access, trust, and disparity
The trauma of centuries of systematic erasure is compounded by a deep disparity in the healthcare available to Native people. Rural Americans already face a growing disparity in access, and the availability of physicians to many Native Americans, particularly in rural areas, is about half the national average. Access equity is one of the primary reasons that WSU founded its health sciences campus in eastern Washington.
Trust is another. “There are more than 500 treaties and virtually every one has been broken,” community health researcher Dedra Buchwald says. Given the history of the relationship, Native Americans and Alaska Natives are understandably reluctant to trust Western institutions.
Researchers, in particular, must deal with a legacy of “helicopter science,” Buchwald says: researchers drop into a Native community, collect the data they think is important, and then leave without so much as a thank you, much less a call-back with results.
Buchwald, a professor of community health and the director of IREACH, the Institute for Research and Education to Advance Community Health at WSU, says that’s why “community-based participatory research is the coin of the realm.” As tribes have become more empowered in recent years, health researchers now work with communities to learn what the communities want. Research, treatment, and intervention projects are conducted in collaboration with Native communities, and all data are shared with them.
But, as Paul points out, it’s not just a matter of getting Native peoples to accept and trust in the ways of Western medicine. Researchers and providers need to respect the vast body of traditional knowledge that indigenous people have developed over millennia. She says health-care providers shouldn’t just practice on a patient; ideally, they practice with the patient, by combining listening skills with cultural competency.
“We have our unique understanding of our health and our culture ways, and how to best listen to a patient,” Paul says. “I strongly feel that we can listen to our own, and a lot of people don’t have that understanding unless you are of our culture. You can have empathy, but I don’t think you can have the full understanding. It’s an issue of trust to be treated by one of your own.”
Although outlawed for centuries, a new sense of respect and appreciation for traditional knowledge is dawning among researchers and practitioners of the Western tradition. Once again, the medicine ways of Natives are being embraced and, as WSU public health researcher Lonnie Nelson says, married to Western medicine to create better healthcare for everybody.
Overcoming disparity through diversity
Nelson’s heritage is rooted in the eastern band of Cherokee Indians, those who resisted relocation to Oklahoma. His mother was a nurse with the Indian Health Service: “We moved around a lot,” living on or near reservations.
“Native Americans and Alaska Natives face a lot of health disparities that find their roots in settler-colonialism and the cultural genocide that has been visited upon our population over the past 200 years. For just about any condition you look at by outcomes and ethnicity, they’ll almost always be worse for Natives,” he says.

Nelson says it is “absolutely true” that having participation of Native practitioners and researchers will help reduce health disparities and improve access. He just took on the position of assistant director for special programs to grow Native initiatives at WSU’s health sciences campus in Spokane. He plans to recruit Native high school students to come to Spokane for six to eight weeks at a time to work with health science researchers. “They’ll see what it’s like to work on campus and do research. They’ll have that exposure to the reality that this is a possible career path for them.
“I am a product of a program very much like that,” Nelson adds. “I was recruited by my tenth grade chemistry teacher and went to Northern Arizona University for a summer to do chemistry.”
Janet Katz, a professor of nursing heavily involved with recruiting and retaining students from communities that are underserved in both education and health-care access, says that changing the admissions criteria for nursing, pharmacy, and medical school from strictly numerical to “mission-driven or holistic admissions” should help draw Native (and other minority) students.
“There’s been a lot of research on this,” she says. “The metrics we use, testing, GPA, have been the main admission criteria, but they don’t necessarily tell you if you have someone with really good critical thinking skills or that they’re going to serve a community and be a good practitioner. So there’s been a move to use those metrics as a screening tool at the beginning, but also certain other criteria, such as life experience. And you base criteria on your mission: What kinds of students do you want to have and to produce? So we might look at what kind of providers we need for Washington state. Do we need more Spanish-speaking practitioners, more low income, more rural? We’re going to do that in nursing next year. The College of Medicine already has that going.”
Daryll DeWald, chancellor of WSU Health Sciences Spokane, affirms this idea: “We want to make WSU Health Sciences an enviable setting for American Indian and Alaska Native students who want to be health-care researchers and practitioners. One of the primary reasons that health disparities still persist in these populations is a shortage of Native physicians, practitioners, and researchers.”
Katz points out that “everybody says we need more diversity among practitioners to provide quality healthcare, but is that really true? And why is that?” In fact, she says, quite a few studies over recent decades show that “ethnic congruence can really alter or affect the interactions that patients have.” In other words, patients who work with practitioners of similar ethnicity, gender, and backgrounds have better outcomes. “That seems to me like a good grounding” and an important part of healing the disparity divide, says Katz.
The majority of healthcare professionals, Katz adds, are white, and in nursing, white women. “So if we want to reflect the population, that needs to change. And that’s what I’ve been involved in, to change that balance. I feel that education is a human right, just as health is a human right. And I don’t want people to not go into healthcare because they grew up in a certain neighborhood or didn’t have a family who could help them. That goes back to the whole idea of social determinants of health: people who are more educated tend to be healthier.” And people who are more educated are often from more affluent families. “It all kind of ties together.”
Part of the solution is role models. Seeing yourself as a doctor or a scientist is often contingent on seeing others like you in those roles. That’s easy for white men; they dominate science, technology, engineering, and medical professions and are more likely to be portrayed in movies, games, and TV as filling those roles. Diversifying the medical and scientific fields requires careful thought; it’s not just a matter of filling seats with faces of diverse hues. What emotional issues will first-generation, minority, or female students face? And how can we design a curriculum that not only empowers a diverse student body but also doubles as ways of ensuring that all gain some level of cultural competency?
Katz has an honors student who is conducting research on Na-ha-shnee, a WSU Health Sciences Spokane program founded by Paul that brings Native high schoolers to campus to experience facets of the health-care professions under the mentorship of WSU’s diverse faculty.

“Participants had a huge commitment to going to college and going into a health career,” Katz says of the students. “They were more confident about their emotional preparedness to go to college before they did the two weeks in Na-ha-shnee.” After the on-campus experience, “they realized they would need a lot of support to be away from home, to study a lot, and to be around people who are different than them.” Katz credits multicultural centers for supplying some of that support, as well as the growing number of Native mentors who are either from local tribes or members of the faculty.
“I got involved in this because of Robbie Paul,” Katz says. “She was the first person on the health sciences campus to start advocating for Native students.” Once that process takes off, it becomes a virtuous cycle: “You get people who go back into their communities. They’ve got a career, an education, and they become role models.”
Paul says WSU is “seen as the leader” in regards to recruiting Native American and Alaska Native students. Since 1995, the efforts of Paul and her team resulted in 67 Natives graduating with bachelors of nursing degrees. And Buchwald’s efforts have resulted in “the country’s biggest and most successful program in regard to training Native researchers: 48 PhDs and MDs, with $200 million in grants.”

After Paul retired, Naomi Bender, a Quechua from Peru by way of Minnesota, was hired as director of Native American Health Sciences. “Only nine or ten medical schools have a focus” on recruiting and training Native students, she says. WSU is joining that group. “Two Native students started in the fall 2019 medical college class.” Because Natives tend to live more collectively than most Americans, Bender says, their inclusion in medical school not only “trains people, but moves and educates entire communities toward healthier outcomes.”
Ways of Knowing
While training Native people in the medical professions and to conduct research in their own communities is critical to healing the health disparities they contend with, everyone could benefit by taking seriously the traditional knowledge of indigenous people.
As Nelson points out, “The word ‘medicine’ does not mean the same thing that it does to Western-thinking individuals. When Natives refer to medicine, they are referring to anything that has an effect on the way you feel: a story, a walk in the woods is medicine. A place may have bad medicine associated with it because someone took their life there. So medicine is not a substance. Western science has a lot to learn from the perspectives of indigenous people.”
“Traditional knowledge,” Buchwald says, “is based on approaches that Native people have been testing for thousands of years. Even though many of their traditional practices have not been vetted in randomized controlled trials, I do think there’s valuable information, both in the methodology, how do you do something, as well in what you do. That value is just beginning to be explored.”
Nelson, who uses talking circles in his intervention and harm-reduction research, explains that, growing up Indian, he “felt a cultural divide between the things I was raised to believe were true and possible and the Western conceptualization of humans: a reductionist, materialist paradigm that posits we are made completely of matter and there is nothing else to us.”
In studying alternative and energy medicine, he discovered “some pretty interesting overlap with the Native worldviews in terms of the connectedness of everything, between people and plants and animals. If you know about those invisible connections, you can interact with them in a certain way that results in better health. And that’s something that could have come out of a Reiki textbook or it could have come out of the mouth of a Native American elder. So I wanted to know if there is any empirical support for those beliefs and conceptualizations.”
Nelson, along with his wife, WSU psychology professor Susan Collins, is beginning a harm-reduction project in Seattle with urban Natives with alcohol use disorders. Central to the project is the use of ceremonial talking circles led by Native healers. The hope is that using such time-tested ways of healing will enable participants to better manage their addictions.
What Nelson, Bender, Buchwald, and Katz are all doing, as Nelson says, is marrying the best of multiple health-care traditions. In parallel with that goal, the operating philosophy of WSU’s health sciences programs is that all students should be trained to work interprofessionally.
Instead of narrow tracks for nursing, pharmacy, and doctors, everyone gets a good dose of their colleagues’ working knowledge. This, too, is a kind of marrying of traditions and, in healthcare, of professions that have been segregated by gender: 75 percent of nurses, for example, are white while 90 percent are female; nearly 70 percent of doctors and surgeons are white. And although the percentage of female doctors and surgeons is increasing rapidly, males still earn, on average, nearly $100,000 per year more than their female counterparts.
Interprofessionalism not only tends to break down the traditional barriers for women and people of color, it also furthers another of WSU’s emerging strengths: incorporating personalized medicine. Personalized, or precision, medicine requires mountains of data on everything from individual genomes and gut biomes to family health history, as well as the people and computing power to analyze and harness it to the betterment of patients. Rather than individual MDs making all or most of the decisions about a course of treatment, WSU’s approach relies on an interprofessional team. The MD may still be at the center of care, using her expertise to guide her team, but in this emerging system patients are more likely to interact directly with health coaches. Coaches listen to their patients, establishing a relationship that has as its goal, as one expert in precision medicine put it, an overall state of well-being attained by preempting disease before it has a chance to manifest.
And this is precisely where at least some Native American traditions have been coming from for centuries. As Kenneth “Bear Hawk” Cohen writes in his book, Honoring the Medicine, healing and curing are not the same. Where Western medicine has traditionally sought to banish disease, indigenous healing seeks a restoration of “well-being and harmony.”
“We’re at a place where we need to think more about how we treat patients,” Bender says. She says we need a better understanding of environmental and cultural factors because, as was her experience growing up among her Quechua family in Peru, “when you’re living in a collective system with access to very few resources, there may be multiple diagnoses of different diseases because of the environment they’re in. And we need practitioners to understand that, to have conversations and get to know their patients more. And I think we’re getting there. But there’s more that we can be doing.”
“There’s a group called the Transcultural Nursing Society,” Katz says. “We’re developing a survey for patients to judge whether their providers are culturally competent or not.” A lot of what constitutes competency is not based on what actions were performed, but how decisions were made; culturally competent practitioners make decisions in tandem with their patients. “It could be any culture” where there is a possibility of a breakdown in communication, Katz adds. “Older people who have young providers,” male doctors working with female patients, and so on.
Acceptance of new ideas, especially in something as critical as healthcare, is never easy. It happens in fits and starts. While some regions and institutions, like Washington state and WSU, blaze innovative trails, people in other regions remain
skeptical.
When asked how he might persuade skeptics to accept the validity and wisdom of traditional knowledge, Nelson becomes very thoughtful before saying, “Anyone who has ever cried at a movie shouldn’t have trouble understanding how a story can affect you. Anyone who’s ever smelled a particular scent that brought them back to their grandmother’s kitchen, shouldn’t have trouble with the idea that burning plants and producing a particular smell in the environment could change the emotional state of people in that environment. Anyone who honestly applies their own experience to their understanding of what can be medicine and what has the ability to change the way that you feel, really shouldn’t have any trouble understanding any of these concepts.”
No one story can heal a broken system, no matter who tells it. As Bender points out, “We have a biased health-care system. There are tribal nations and voices that can help us move the dial” to heal our system. “And, as a land-grant institution, we should be doing that.”
Paul says her father “always told me, ‘We need to learn to listen, and to listen to learn.’” Native Americans greatly value silence and know there are more voices than just those of people. “My dad knew how to listen to birds to predict the weather,” she says. “How do you do that?” she’d ask him. He’d chuckle and say, “You have to have a strong spirit guide, but you also have to learn to listen quietly.”
As a paradigm for healing disparity, listening is certainly a good place to begin. “My father never preached, he just gave me a story,” Paul says. “Ninety percent of healing is being listened to. You have to learn to listen so quietly that you can hear a bird taking a drink on the other side of the mountain.”
Web extras
Flour Sacks: A Memoir by Naomi Bender